
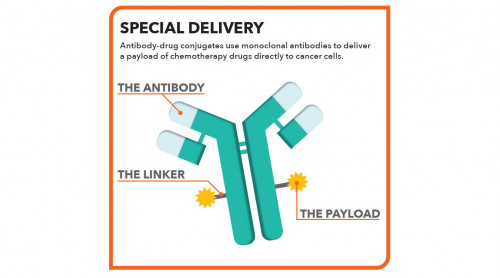
The antibody-drug conjugate Enhertu (fam-trastuzumab deruxtecan, or T-DXd), which was initially approved for metastatic breast cancer with high HER2 expression, also works well for patients who have tumors with low or ultralow HER2 levels, according to study results presented this week at the American Society of Clinical Oncology Annual Meeting (ASCO 2024) in Chicago.
In the Phase III DESTINY-Breast06 trial, Enhertu extended progression-free survival (PFS) by about five months compared with standard chemotherapy, reducing the risk of disease progression or death by 37%.
“With a median progression-free survival of more than a year, the results from DESTINY-Breast06 show that Enhertu could become a new standard of care for patients with HER2-low and HER2-ultralow expressing tumors following endocrine therapy in the metastatic setting,” said lead investigator Giuseppe Curigliano, MD, PhD, of the University of Milan.
Breast cancer is classified by the type of receptors on tumors. Most have estrogen or progesterone receptors that make them treatable with hormone therapy, classified as HR-positive. Around 15% to 20% of breast tumors have a high level of HER2, a receptor for a protein that promotes cell growth, classified as HER2-positive. However, around 60% of people traditionally classified as HER2-negative actually have tumors with some HER2 receptors, now classified as HER2-low, and perhaps another 25% may be HER2-ultralow. Triple-negative breast cancer doesn’t express any of these receptors and is harder to treat.
These results “represent a potential shift in how we classify and treat metastatic breast cancer, as we may have the opportunity to use trastuzumab deruxtecan earlier in the treatment of HR-positive metastatic breast cancer and expand trastuzumab deruxtecan into new metastatic breast cancer patients who previously have not been able to benefit from a targeted medicine post-endocrine therapy,” Curigliano said.
Results from the Phase II DESTINY-Breast01 study, published in 2019, showed that Enhertu extended progression-free survival for people with HER2-positive inoperable or metastatic breast cancer who previously used the older ADC Kadcyla (trastuzumab emtansine, or T-DM1). This led to accelerated approval of Enhertu later that year. DESTINY-Breast02, published in 2023, found that Enhertu more than doubled progression-free survival compared with chemotherapy for previously treated patients with HER2-positive advanced breast cancer.
The Phase III DESTINY-Breast04 trial, presented at ASCO 2022, showed that Enhertu improved both progression-free survival and overall survival compared with chemotherapy for previously treated people with either HER2-positive or HER2-low advanced breast cancer. The Food and Drug Administration approved Enhertu for HER2-low breast cancer that August. The drug has also been approved for HER2-positive stomach cancer and, this April, for all inoperable or metastatic HER2-positive tumors regardless of location.
DESTINY-Breast06 focused on HR-positive metastatic breast cancer patients who previously would have been classified as HER2-negative. The study included 713 participants with HER2-low tumors (a score of +1 or +2) and 153 with HER2-ultralow tumors (a score of 0 but detectable). The median age was approximately 58 years.
The participants had received no prior chemotherapy for advanced disease, but they had used at least two lines of prior hormone therapy or one line of hormone therapy plus a CDK4/6 inhibitor or had experienced rapid disease recurrence despite adjuvant hormone therapy. They were randomly assigned to receive Enhertu by IV infusion once every three weeks or chemotherapy (capecitabine, paclitaxel or nab-paclitaxel).
Enhertu demonstrated a statistically significant and clinically meaningful improvement in progression-free survival after a median 18 months of follow-up. Enhertu reduced the risk of disease progression or death by 38% compared with standard-of-care chemotherapy in the HER2-low group, with median PFS times of 13.2 months versus 8.1 months. In an exploratory analysis of the smaller HER2-ultralow group, Enhertu decreased the risk of disease progression or death by 22%, with median PFS times of 13.2 months versus 8.3 months, respectively.
The objective response rate, or tumor shrinkage, was nearly twice as high with Enhertu compared to chemotherapy (57% versus 31%). Nine patients in the HER2-low group and four in the HER2-ultralow group experienced complete responses, but none in the chemotherapy group did so. One-year overall survival rates were approximately 88% for the HER2-low group, 84% for the HER2-ultralow group and 80% for the chemotherapy group, but these data are not yet mature.
Side effects were common in both treatment groups. About 40% of Enhertu recipients and about 30% of chemotherapy recipients experienced serious adverse events. Nausea was the most common side effect in the Enhertu group and the most frequent reason for discontinuation. The most common severe (Grade 3 or higher) treatment-related adverse events were neutropenia (21%), low white blood cell counts (7%) and anemia (6%). Forty-nine people (11%) developed interstitial lung disease (ILD) or pneumonitis, a type of lung inflammation. This was usually mild to moderate, but there were three severe ILD events and three deaths. Overall, people in the chemotherapy group were more likely to stop treatment due to disease progression, side effects or other reasons.
“In comparison to standard chemotherapy, trastuzumab deruxtecan significantly improved progression-free survival, with similar results in both HER2-low and HER2-ultralow disease. These data suggest that trastuzumab deruxtecan may become a preferred first-line treatment option for most patients with HR-positive metastatic breast cancer after progression on endocrine therapy,” Erica Mayer, MD, MPH, of Dana-Farber Cancer Institute, said in an ASCO news release. “It is important to note, however, that trastuzumab deruxtecan resulted in more serious toxicities compared to traditional chemotherapy and may not be the right choice for every patient.”
Researchers also presented interim results from the Phase I/IIb DESTINY-Breast07 trial, which is evaluating Enhertu alone or in combination with other therapies as a first-line treatment for people with HER2-positive metastatic breast cancer. So far, the study has demonstrated an overall response rate of 76% for Enhertu monotherapy and 84% for Enhertu plus Perjeta (pertuzumab). One-year progression-free survival rates were 81% and 89%, respectively. Safety profiles were consistent with those seen in prior studies.
The Phase III DESTINY-Breast03 trial showed that Enhertu delayed disease progression and improved overall survival more than Kadcyla in patients with HER2-positive metastatic breast cancer who previously used Herceptin and chemotherapy. Updated results presented at this week’s meeting showed that Enhertu continues to demonstrate “a clinically meaningful survival improvement” over Kadcyla after more than three years of follow-up, according to an AstraZeneca press release. The DESTINY-Breast05 study is comparing Enhertu versus Kadcyla as adjuvant therapy after surgery for people with HER2-positive early breast cancer.
Taken together, these findings—along with several other presentations at the meeting— demonstrate that antibody-drug conjugates are becoming a mainstay of treatment for multiple types of advanced cancer, and they may soon be options for earlier-stage cancer as well.
Click here for more news about breast cancer.
Click here to learn more about antibody-drug conjugates.
Click here for more news from ASCO 2024.




Comments
Comments